In the vast majority of cases, vitiligo is diagnosed clinically, on clinical examination alone, possibly with a Wood’s lamp, without the need for a skin biopsy.
It is important to explain the disease to the patient. It is an autoimmune pathology for which curative treatments are being developed or obtained an MA (e.g. topical JAK inhibitors). There is no contraindication to sun exposure, but it increases the visibility of the disease.
Contrary to popular belief, vitiligo is not a psychosomatic disease but must be considered as a serious dermatosis because of the often significant psychosocial impact it causes. This dermatosis should therefore not be considered a “minor cosmetic problem”.
Clinical examination
The clinical diagnosis of vitiligo is mainly based on the observation of the characteristic physical signs, as well as on the medical examination of the patient. Here are the main steps:
1. History (Medical History)
- Symptoms : Identification of depigmented areas of skin, often symmetrical and white in color, without other symptoms such as itching.
- Family history : Vitiligo sometimes has a genetic component. The doctor may ask if other family members are affected.
- Associated conditions : Some autoimmune diseases, such as thyroid disorders, may be associated with vitiligo.
2. Physical examination
- The doctor examines the depigmented spots on the skin. Vitiligo is characterized by sharp white spots, often with a well-defined border.
- Ultraviolet lamps (Wood’s lamp): This device helps detect areas of depigmentation by making them more visible under ultraviolet light. The vitiligo spots glow white in this light. detects melanocytic loss and intensity of depigmentation (very white and not gray lesions as in hypopigmentation), especially if light phototype or in weakly pigmented areas of dark-skinned subjects (palmoplantar regions).
3. Exclusion of other causes of depigmentation
- Differential diagnosis is important to rule out other conditions like pityriasis versicolor, post-inflammatory leukoderma , or toxic causes.
4. Additional Testing
- Skin biopsy (rarely needed): May be performed to confirm the absence of melanocytes in the affected skin.
- Blood tests : To look for associated autoimmune diseases (e.g., thyroid assays, thyroid antibodies).
5. Photographs for follow-up
- Photographs of the affected areas can be taken to track the evolution of vitiligo over time.
This approach makes it possible to make an accurate diagnosis and determine the most appropriate treatment plan.
THREE MAIN FORMS
01
non-segmental
Bilateral and often symmetrical hypochromic macules : Depigmented spots appear on both sides of the body, often symmetrically.
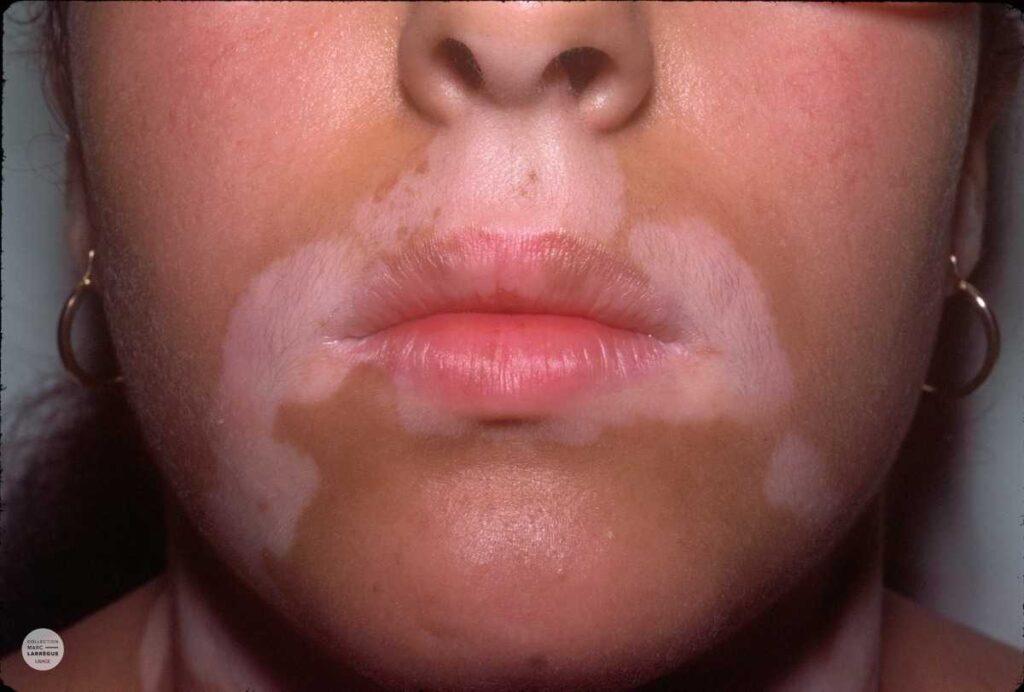
Acrofacial distribution : Lesions occur mainly on the hands, feet, and around the orifices of the face (peri-orificial). They can also be dispersed symmetrically over the entire body and evolve in flare-ups.
Koebner’s phenomenon : The topography of the lesions can correspond to areas subject to friction or pressure.
Hair change : In the affected areas, the hair, initially pigmented, gradually turns white.
02
Segmental vitiligo
Unilateral distribution : Lesions usually appear on only one side of the body and follow a segment of skin corresponding to a dermatome (area innervated by a nerve).
Early onset : It often appears earlier than other forms of vitiligo, mainly in children and young adults.
Rapid evolution but stabilization : Unlike non-segmental vitiligo, this form evolves rapidly at first, then tends to stabilize and does not extend beyond the initially affected area.
Absence of Koebner’s phenomenon : Lesions are usually not influenced by friction or pressure, unlike non-segmental vitiligo.
Associated with white hair : As with non-segmental vitiligo, the hairs in the affected areas can also turn white.
Different response to treatments : Segmental vitiligo often responds better to treatments such as skin grafting or surgical techniques because it is more localized and stable.
03
Vitiligo universalis
This is a very rare form where almost the entire surface of the body is depigmented, often more than 80 to 90% of the skin.
Treatment
The management of vitiligo is based on several therapeutic options, adapted to the course of the disease and the impact felt by the patient. Here is a comprehensive overview by combining local and systemic strategies, as well as psychological support options.
1. Topical treatments
- Dermocorticoids : Depending on the extent and discomfort, topical corticosteroids with high activity (betamethasone 0.05%) or very strong activity (clobetasol 0.05%) such as Dermoval® or Clarelux® can be applied daily for a limited time (2 to 3 months). They are particularly effective on the areas outside the face and neck.
- Calcineurin inhibitors (tacrolimus, pimecrolimus): Tacrolimus 0.03% or 0.1% : Used as an ointment, it is often prescribed for the face. Although it does not have specific marketing authorization for vitiligo, it offers an alternative to corticosteroids with fewer long-term side effects, especially on sensitive areas such as the face.
2. Phototherapy
- Narrow-spectrum UVB (TL-01): UVB-NB phototherapy is an effective option, especially for extensive forms of vitiligo. It can be combined with systemic corticosteroids in the case of rapidly extensive vitiligo, stopping the progression of the disease and promoting repigmentation in more than half of patients.
- PUVA : Used less frequently today, it combines psoralens and UVA exposure to stimulate pigmentation. It is reserved for refractory cases because of its potential side effects (skin aging, skin cancer).
3. Systemic therapies
- Systemic corticosteroids : In case of rapid progression, the use of oral or injectable corticosteroids, in combination with UVB phototherapy, may help to slow the spread of the disease.
4. Surgical therapies
- Skin or melanocyte grafts : Used mainly for segmental or localized forms. They are offered when other treatments are ineffective or the lesions are stable.
5. Camouflage and beauty treatments
- Cosmetological products : Specialized covering creams such as Viticolor gel® or self-tanners can be offered to camouflage white spots and improve the appearance. Dermopigmentation (medical tattooing) is also an option for certain visible areas such as the face or lips.
- Cosmetic Solutions : These solutions help restore self-esteem and are important when medical treatments do not yield quick results.
6. Psychological support and accompaniment
- French Association of Vitiligo : It is essential to suggest that the patient get in touch with this association, which offers support groups, telephone assistance, social support networks, newsletters and information days to share experiences and find support.
- Psychological therapies : Since vitiligo has a significant psychosocial impact, psychological support or cognitive behavioral therapy can be helpful in managing the stress and anxiety related to the disease.
7. Other Treatments and Development
- JAK inhibitors : New targeted therapies are in development and show promising results for some forms of vitiligo.
- Total depigmentation : For very extensive forms, complete depigmentation of the remaining skin may be considered in order to even out the body color.
Conclusion
The management of vitiligo should be individualized, with a combination of topical, systemic, aesthetic and psychological treatments depending on the course of the disease and the patient’s preferences. Regular follow-up with a dermatologist allows strategies to be adapted over time.
