Superficial cutaneous fungus with dermatophytes belonging to the genera Trichophyton, Microsporum and Epidermophyton (in France: T. rubrum (70%), T. interdigitale (15%), E. floccosum (5%) and M. canis (5%)).
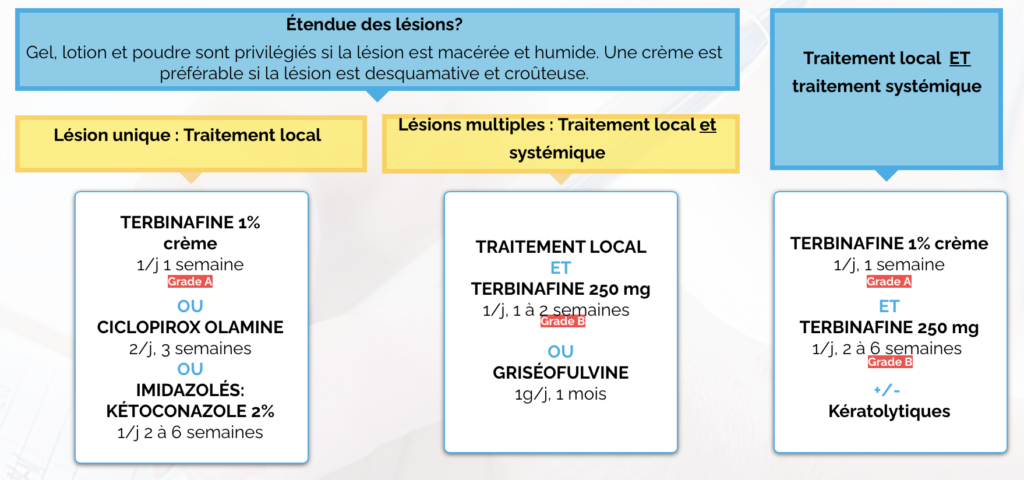
If only one or two limited lesions are found, local treatment is usually sufficient.
Terbinafine is the most active antifungal on dermatophytes.

Patient advice
- To avoid recurrences and relapses: dry the feet and folds (with a hairdryer if necessary).
- Disinfect reseeding stoves : application of antifungal powder in slippers, barefoot shoes, on bathroom mats, etc.
- Washing shower trays and tiles with bleach.
- Treatment of all family members with dermatophytis.
- In the event of usual attendance at sports clubs or collective changing rooms and showers, it is recommended to wear flip-flops or sandals as well as hygiene and careful drying of the feet and the possible application of antifungals (powder for example) on these days.
- Chronic hyperhidrosis should be treated.
Treatments
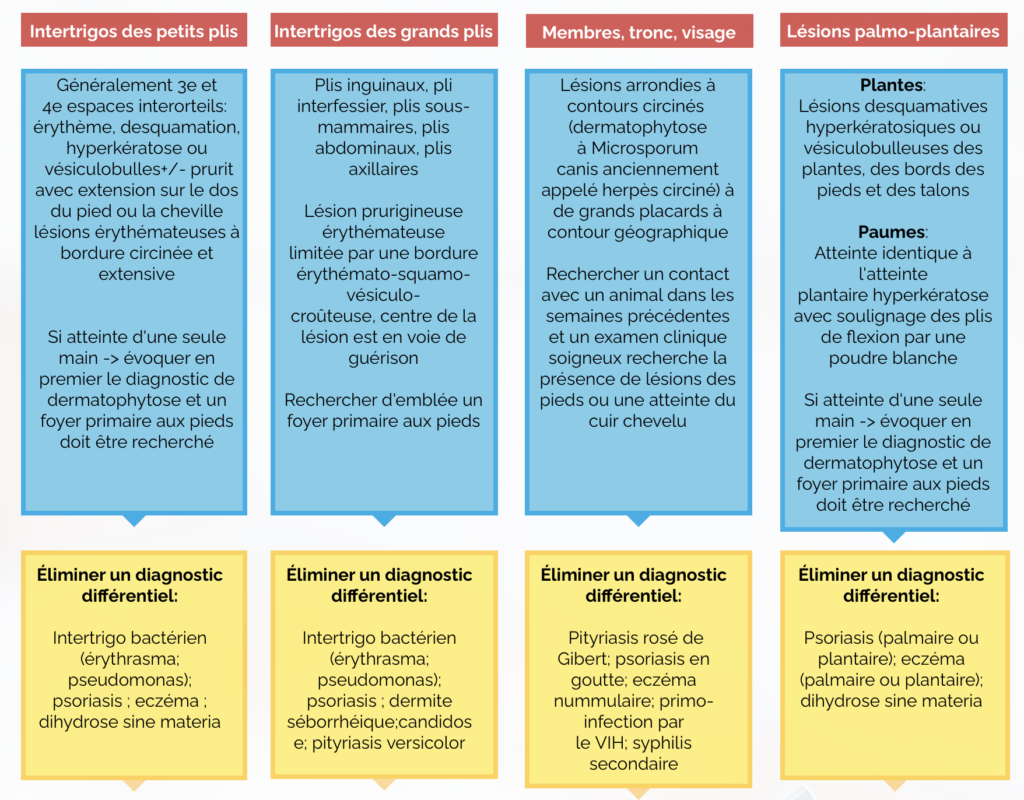
Even if here the clinical presentation of dermatophytosis of the hairless skin (or circinated herpes) is typical, the diagnosis must be confirmed by a systematic mycological sample (mycological sampling of scales from the periphery).
In the case of this single lesion, treatment consists of local treatment (which can be started before the results of the sample) by:
- Terbinafine 1% cream (most active on dermatophytes) once daily for 1 week;
- Or ciclopirox olamine 1% 2 times daily for 3 weeks;
- Or ketoconazole 2% once daily for 4 to 6 weeks depending on clinical course.
It is also important to fight against the contributing factors : heat, humidity, local trauma, occlusion of folds, immunosuppression, diabetes, etc.
We must look for a notion of contending (between humans or animals). Epidemiological investigation is therefore essential, with veterinary care of the contaminating animal and/or screening and treatment of colonized contact subjects.
Pickup