CONTEXT
Melanoma is an uncommon cancer compared to epithelial carcinomas but it is the most serious of the malignant skin tumors because its ability to metastasize is life-threatening.
There are strong arguments for promoting early diagnosis among the public and all health professionals: in 2006, treatments for metastatic melanoma had no effect on mortality. Only the diagnosis of melanoma in situ (early stage of melanoma) and melanomas of low thickness (measured by the Breslow index) could reduce mortality related to this cancer.
The data in the literature show that the patient’s prognosis depends on the value of the Breslow index and the presence or absence of ulceration on histological examination at the time of melanoma excision:
- an inverse correlation between the Breslow index and survival after treatment is observed: the 5-year survival rate is 91-95% when this index is < 1 mm and is 63-79% when it is between 2 and 4 mm;
- the rate of local, regional or distant recurrences is correlated with the Breslow index.
The treatment will be all the more effective if it is applied to melanoma with a low Breslow index: effectiveness on mortality and/or recurrence rate. Campaigns to encourage early diagnosis have a positive impact (increase in the number of melanomas detected and decrease in the thickness of melanomas that have been removed)
THE DIFFERENT TYPES OF MELANOMA
- Melanoma with superficial extension (SSM): a spot with an irregular polycyclic outline, of polychrome inhomogeneous colour (black, brown, red, achromic), non-palpable or palpable depending on its phase of evolution. Slow growth (months to years) 70-80% of melanomas.
- Nodular melanoma (NM): black (sometimes achromic) nodule, firm, rounded, which may ulcerate, crust, ooze or bleed. Rapid growth (weeks to months) 4-18% of melanomas.
- Dubreuilh’s melanoma: pigmented, inhomogeneous spot, ranging from black to dark brown, observed on photo-exposed areas in the elderly (mainly face).
- Acram-lentiginous melanoma: observed on the palms or soles (brown or black spot with irregular outline), nails (melanin > band 6 mm wide, irregular pigmentation), skin areas not exposed to the sun.
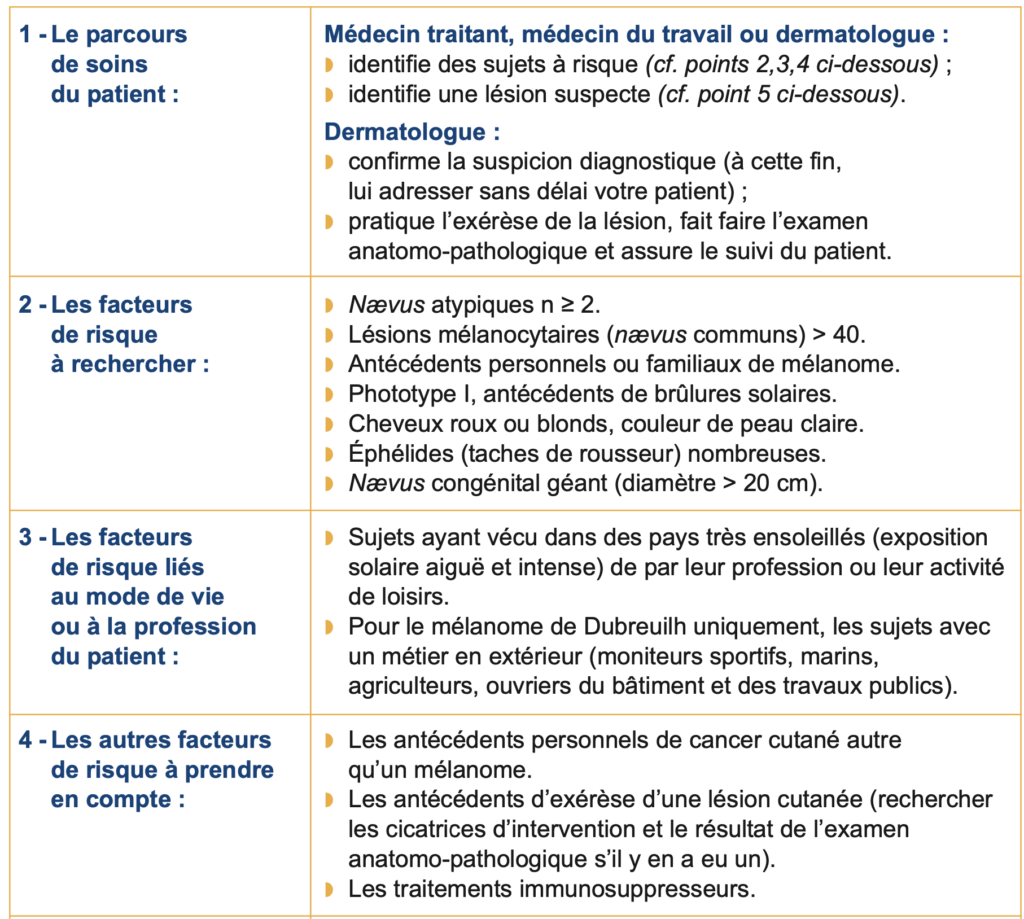
RISK FACTORS TO LOOK FOR
The following factors increase the risk (doubled risk) of developing melanoma (for details of these factors, see the table on the last page):
- numerous common nevi (moles), atypical nevi ;
- lifestyle with intense sun exposure;
- history of sunburn (sunburns);
- type I skin phototype (sunburn + absence of tanning);
- personal or family history of melanoma;
- physical characteristics (hair or skin color, ephelides).
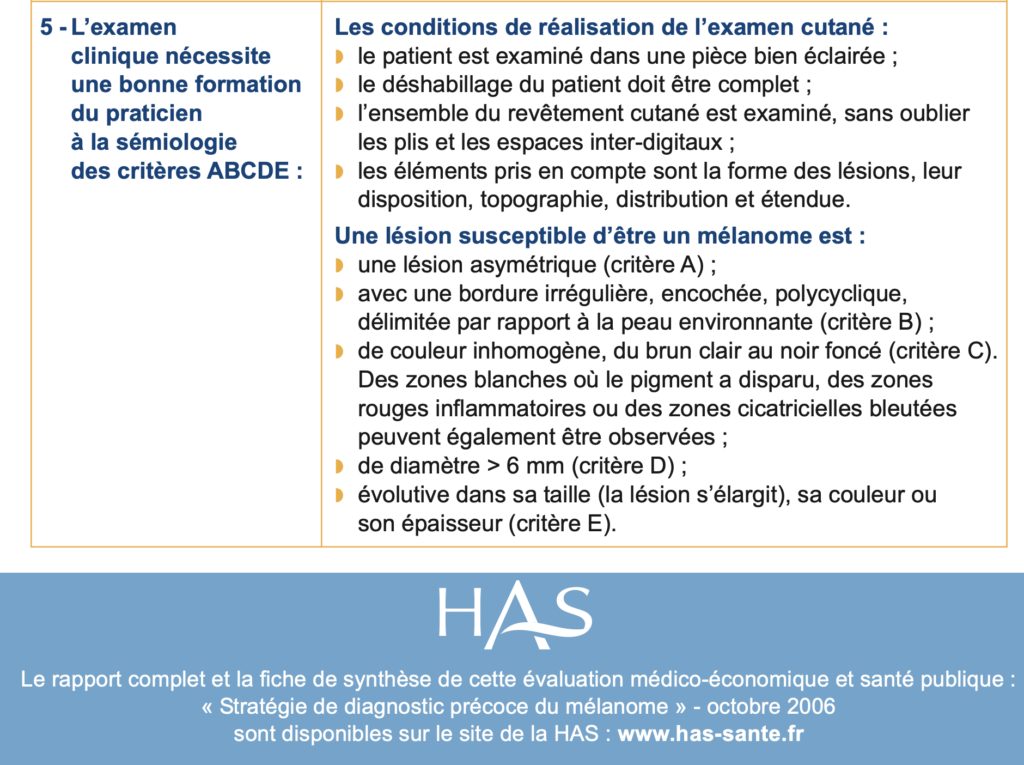
CLINICAL EXAMINATION
The stage of severity of melanoma cannot be known solely from the clinical aspect (no correlation between the diameter of the melanoma and its thickness). The clinical examination is an effective method provided that you know the semiology of melanomas (importance of training).
The visual analytical approach
- The ABCDE rule is the reference method in France.
- The acronym ABCDE stands for: A = asymmetry; B = edge; C = color;
- D = diameter; E = scalability (see table on the last page).
- A melanocytic lesion is considered suspicious if two of these criteria are validated (criterion E being the most relevant criterion).
The visual cognitive approach
- In a given subject, the nevi have a homogeneous clinical appearance (the nevi resemble each other).
- A melanocytic lesion is considered suspicious if it is clinically different from the patient’s other nevi in shape, color, or thickness.
YOUR PATIENT’S COORDINATED CARE PATHWAY
If you have identified a patient at risk for melanoma, you must:
- encourage them to have their skin examined once a year by a dermatologist;
- encourage them to have a skin self-examination once a quarter (see below);
- inform him about the risks associated with sun exposure.
If you have identified a suspicious lesion in a patient at risk or not, you must refer your patient to a dermatologist without delay:
- if the dermatologist confirms the suspicion of melanoma, he will perform an excision of the lesion;
- the anatomical pathological examination will confirm or not the diagnosis of melanoma;
- Depending on the results of this examination, the dermatologist will decide on the therapeutic management (treatment, monitoring) and explain it to your patient.
SKIN SELF-EXAMINATION: WHY? HOW?
Self-examination allows your patient to examine their entire skin on their own (completion time: 15 minutes). Your patient will need to look for a melanocytic lesion that is clinically different from their other nevi or that is recent or progressive in size, color, or thickness.
- Step 1 : Direct examination: the patient should examine with the naked eye the palms of their hands and feet, their nails, fingers and the spaces between the fingers of their hands and feet, the front of their arms and forearms, their thighs and legs.
- Step 2 : The full-length mirror examination: the patient will have to stand in front of a vertical foot-mirror and examine his skin from top to bottom. He will turn the left and then the right side of his body towards the mirror, with his arms raised vertically.
- Step 3 : Examination with a hand-held mirror: for areas of skin that are not accessible to the eye, the patient can use a hand-held mirror. Sitting on a stool, he raises each leg to examine the internal, external and posterior aspects of the calf and thigh. The posterior aspect of the arms, neck, back, scalp and genital area will also be examined using the hand mirror. The patient can also ask for help from someone close to him.